By Patrick Cooney, for AMRC

FEDERAL AGENCY NEWS
AMRC Visits with FDA’s Center for Clinical Trial Innovation
On June 10, 2026, AMRC representatives met with staff from the Food and Drug Administration to discuss the agency’s efforts to innovate in clinical trial design.
Th Center for Clinical Trial Innovation (C3TI) was launched in 2024, as a central hub within the Center for Drug Evaluation and Research (CDER) to support the implementation of innovative approaches to clinical trial design and conduct. Its mission is to promote existing and future clinical trial innovation through enhanced communication and collaboration — both internally across CDER’s offices and externally with sponsors, patient advocates, and the research community.
C3TI operates through three primary functions:
- Knowledge sharing: C3TI maintains a searchable knowledge repository called C3TI Compass — a centralized platform for information on clinical trial innovation activities, including lessons learned, guidance documents, and workshop outputs.
- Cross-CDER collaboration: C3TI serves as the connective tissue across CDER’s diverse innovation programs, including Complex Innovative Trial Designs (CID), Model-Informed Drug Development (MIDD), Rare Disease Endpoint Advancement (RDEA), Digital Health Technologies, and Real-World Evidence initiatives.
- The Demonstration Program: C3TI manages a structured demonstration program that offers sponsors of innovative trials early, enhanced engagement with CDER leadership across multiple offices, including the Office of Medical Policy, Office of New Drugs, and Office of Translational Sciences.
C3TI is governed by leadership from the Office of the Center Director alongside those operational offices. The program accepts up to nine proposals on a rolling basis within a 12-month period — a deliberately limited cohort designed to ensure meaningful, high-quality CDER engagement with each participating sponsor.
The agency recognizes that while guidance documents have been essential tools for encouraging trial innovation, real-world examples are what actually move the needle on adoption. C3TI demonstration projects are intended to serve as those case examples — building an empirical track record that can inform guidance updates and broaden the innovation ecosystem.
The C3TI Demonstration Program currently operates three project areas. Each targets a distinct dimension of trial innovation. The June 10th meeting with AMRC focused on one of those projects: Streamlined Trials Embedded in Clinical Practice (STEP).
Streamlined Trials Embedded in Clinical Practice
Pragmatic and point-of-care trial designs that integrate research into routine clinical settings.
- Targets trials with limited procedures outside routine clinical care, decentralized trial delivery, and use of real-world data (RWD) for outcomes.
- CDER engagement focuses on resolving statistical analysis questions, real-world data/evidence integration, endpoint selection, and inspectional approaches.
- Designed for trials that are more resource-efficient, recruit broader and more diverse populations, and can complete enrollment more rapidly — all critical advantages in rare cancer settings.
- Participating sponsors receive enhanced engagement from CDER’s Office of Medical Policy, Office of New Drugs, and Office of Translational Sciences, with access to leadership across these offices.
- Lessons learned are shared publicly and inform updates to relevant CDER guidance documents, amplifying the impact of each participating trial.
- Connects directly to CDER’s broader “Integrating Randomized Controlled Trials for Drug and Biological Products Into Routine Clinical Practice” guidance initiative.
AMRC’s meeting with the CDER C3TI team surfaced that they are interested in finding their first sponsor to initiate the STEP project.
The STEP demonstration project may be one of the most consequential C3TI initiatives for rare cancer sponsors. The structural challenges of rare cancer trials — geographically dispersed patients, low disease incidence, and the burden of travel to specialized research centers — map directly onto the pragmatic design elements STEP is designed to support. The ability to decentralize trial procedures, use real-world data for outcome capture, and integrate research into point-of-care settings addresses core barriers that have historically limited rare cancer trial enrollment.
C3TI’s demonstration projects are distinct from existing programs like Complex Innovative Trial Designs (CID) or Rare Disease Endpoint Advancement (RDEA). While those programs explore and qualify specific innovations, C3TI’s role is to streamline the process of collaboration between CDER experts, review teams, and sponsors — and to expand the breadth of innovations explored. An open application window allows proposals as early as trial conception, well before a sponsor has fully developed a protocol.
Sponsors are expected to share select details of their trials and innovations as they progress, starting from the finalization of study design. This includes updates, lessons learned, and relevant insights, with confidentiality protections for proprietary information. The expectation of knowledge sharing is by design: each demonstration project is intended not only to benefit the participating sponsor, but to build a body of precedent and experience that the broader community can draw on.
AMRC members interested in engaging with C3TI can find more information at this link. Please let us know if you decide to reach out to them.
If you know of a sponsor that would be interested in talking with the CDER team, AMRC can help by putting you in touch with the proper staff. AMRC will continue its dialogue with CDER on C3TI and will monitor the evolution of the program’s demonstration projects, knowledge repository, and guidance outputs.
CAPITOL HILL NEWS
FY2027 Funding for Health Research
President Trump’s FY2027 Budget Request, released in early April 2026, proposed an overall U.S. Health and Human Services (HHS) budget of $111.1 billion — a 12.5% reduction from FY2026 enacted levels. For health research agencies specifically, the proposed cuts were severe and would represent a fundamental reshaping of the federal biomedical research enterprise.
Congress, however, has a different vision and has largely rejected the Trump budget for HHS. The House Appropriations Committee released its FY2027 Labor, Health and Human Services, Education, and Related Agencies (Labor-HHS) bill on June 4, 2026. The bill was approved by the Committee on June 9, 2026. Subcommittee Chairman Robert Aderholt (R-AL) characterized the bill as one that “prioritizes biomedical research, biodefense, and rural health.”
The bill provides a total discretionary allocation of $189.3 billion — $5.6 billion (3%) below FY2026 enacted levels — but significantly diverges from the President’s Budget on health research priorities:
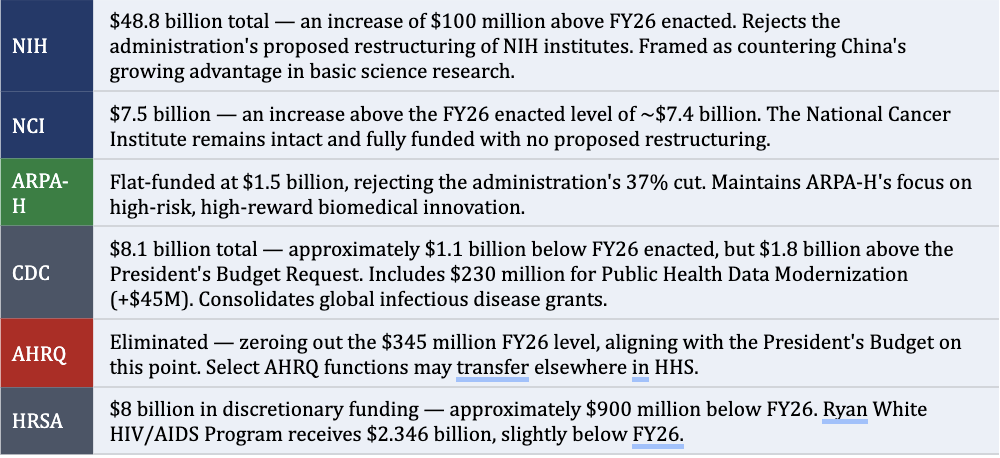
Notably, the House bill does not adopt the President’s proposed HHS restructuring, including the consolidation of NIH institutes, signaling that Congress remains cautious about large-scale reorganization of research infrastructure, even from members of the President’s own party.
The Senate Appropriations Committee has not yet released its FY2027 Labor-HHS bill, and Senate action is not expected until late summer at the earliest. The House bill passed committee along party lines, which typically signals a more difficult floor passage and a longer conference negotiation with the Senate.
Congress faces a September 30, 2026, deadline to enact FY2027 appropriations. Given the wide gap between the House and Senate visions — and the experience of FY2026, when a government shutdown preceded a February 2026 omnibus — a Continuing Resolution (CR) extending into late 2026 or early 2027 is a realistic outcome.
